what term is used to describe the portion of the graph where the waves overlap
ECG Estimation Part i: definitions, criteria, and characteristics of the normal ECG (EKG) waves, intervals, durations & rhythm
This is arguably i of the nigh important chapters throughout this course. At the heart of ECG interpretation lies the ability to determine whether the ECG waves and intervals are normal. This chapter will focus on the ECG waves in terms of morphology (appearance), durations and intervals. A rather extensive discussion is provided in club to give the reader firm knowledge of normal findings, normal variants (i.e less common variants of what is considered normal) and pathological variants. Thus, in this affiliate, you will learn the physiological ground of all ECG waves and how to determine whether the ECG is normal or abnormal. Although heart rhythm will be discussed in particular in the next capacity, fundamental aspects of rhythm will also be covered in this discussion (refer to Normal Rhythm and Arrhythmias). Also annotation that this affiliate is accompanied by a video lecture: Video lecture: The Normal ECG, which covers all topics discussed below.
-
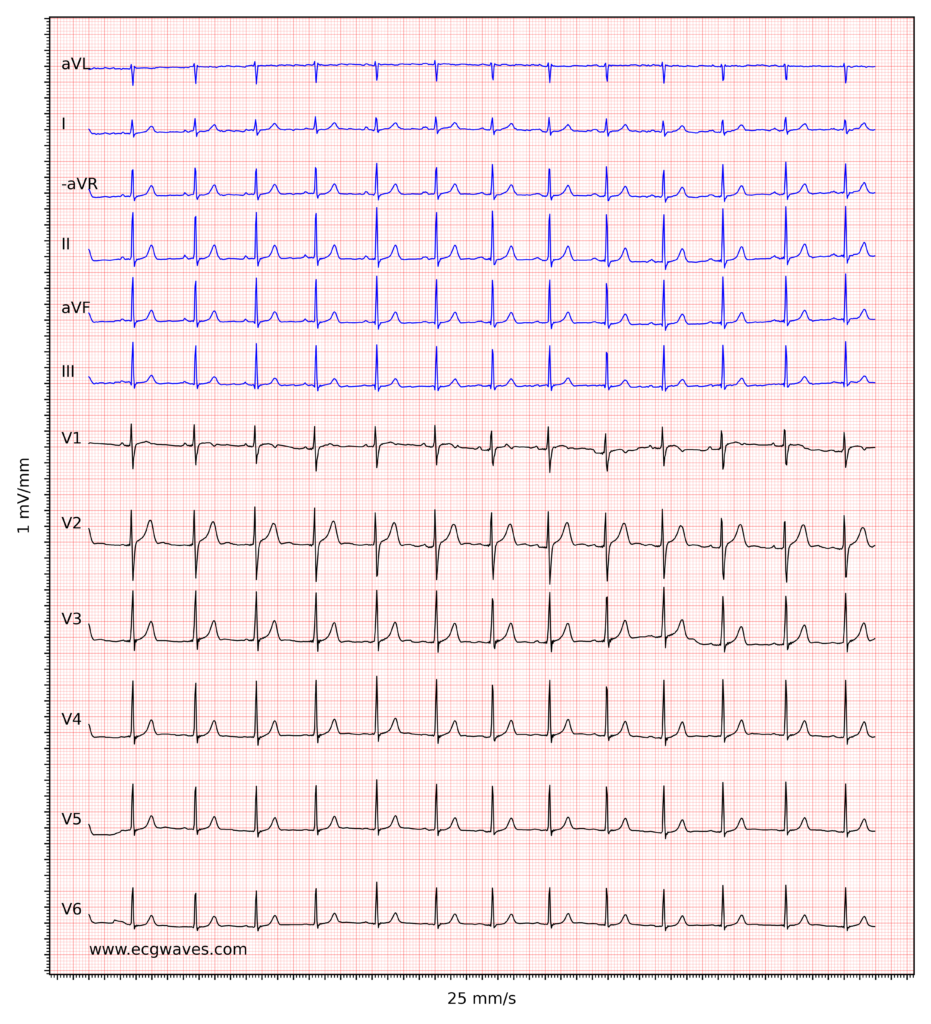
ECG example i. Normal sinus rhythm. -
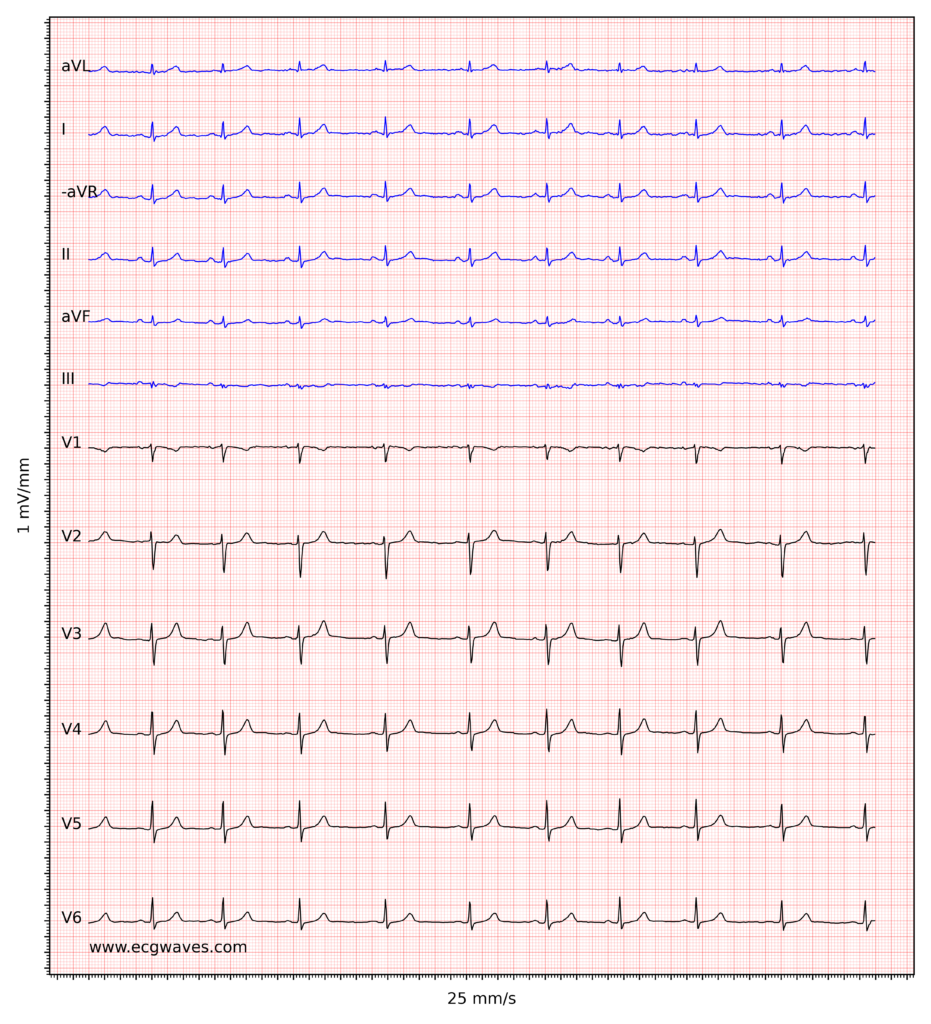
ECG example ii. Normal sinus rhythm. R-waves have low amplitude, suggesting low voltage (see below). -
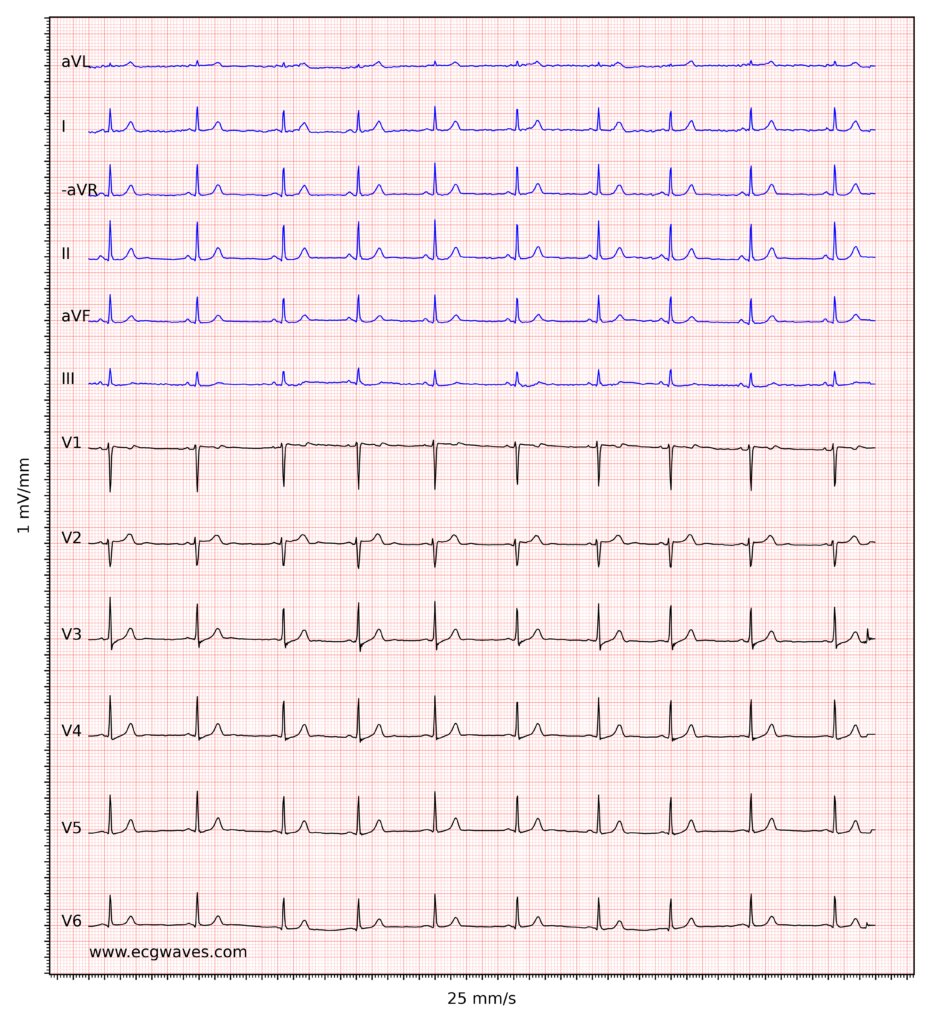
ECG example iii. Normal sinus rhythm. -

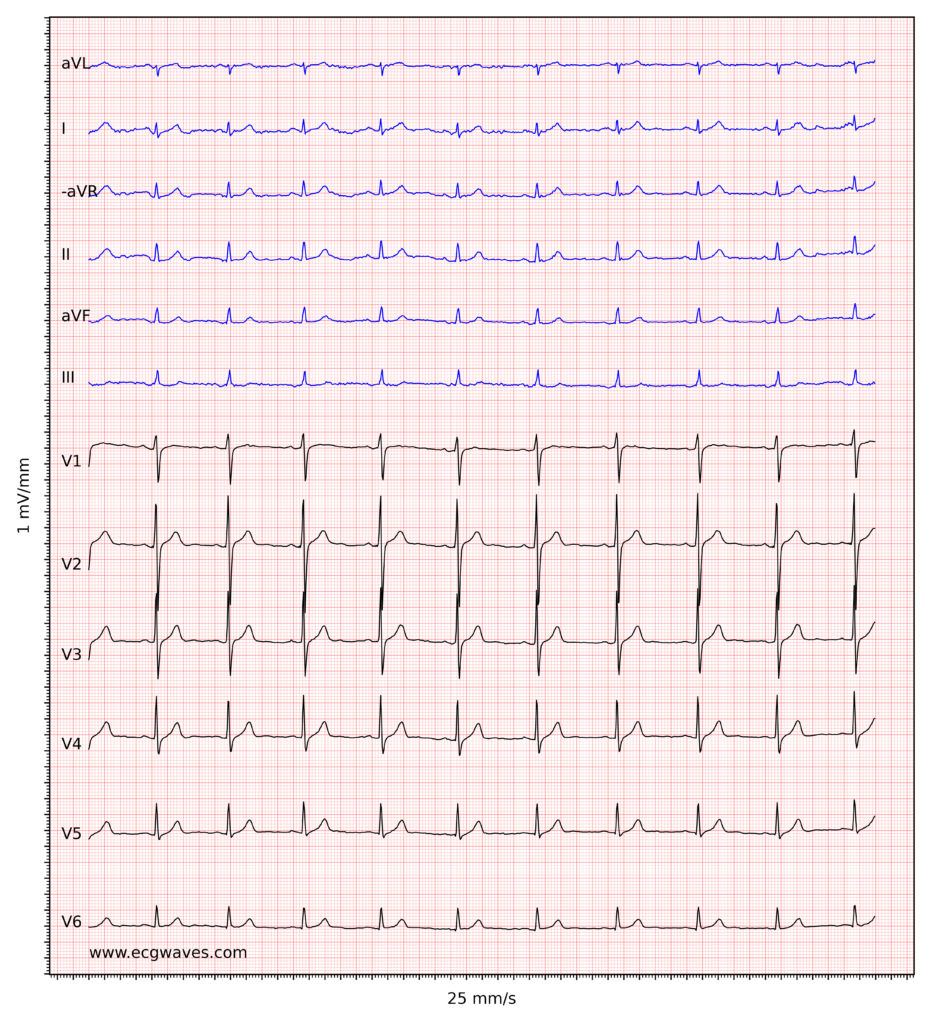
ECG example 4. Normal sinus rhythm. -

ECG instance 5. Sinus rhythm. Negative T-waves in leads aVF and III. Discrete ST-segment depressions in leads V5-V6. -
ECG example half dozen. Sinus rhythm, rapid progression of R-waves in precordial leads. Slight ST-segment elevation in leads V2-V3, which is normal in men and women. -
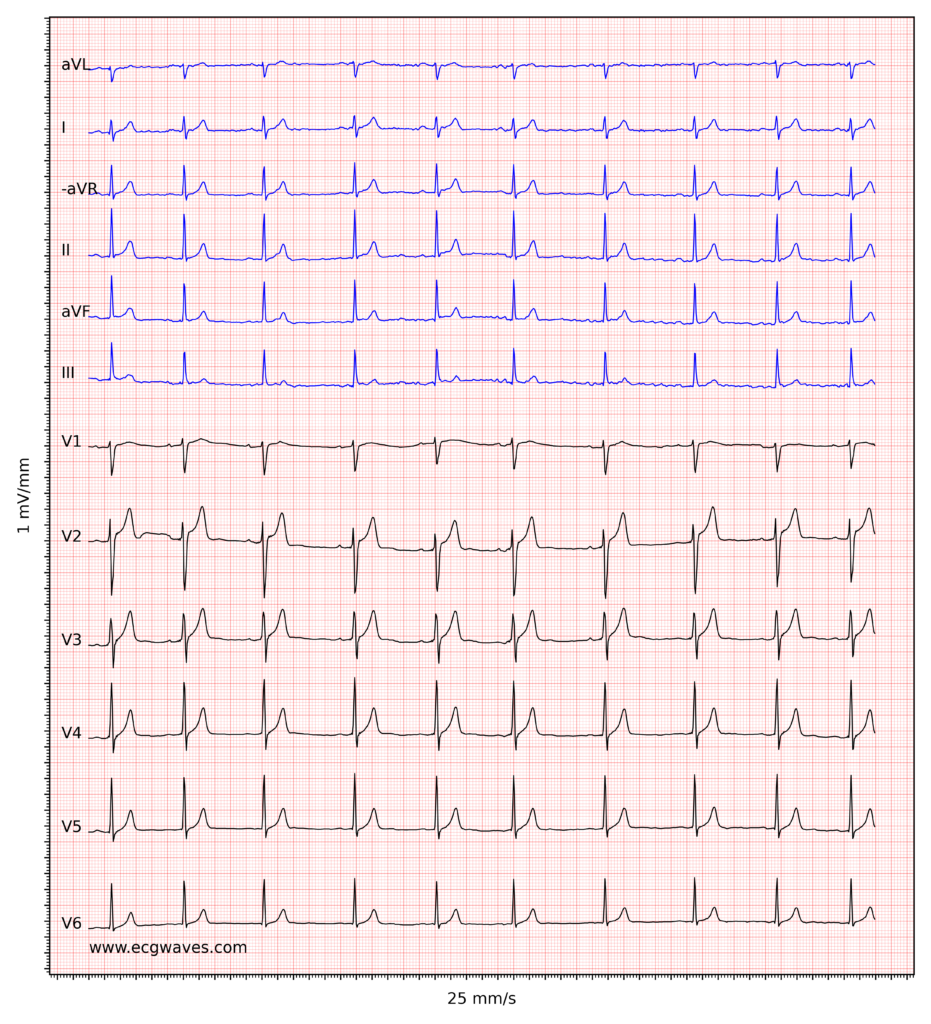
ECG example 7. Sinus rhythm. Relatively large T-waves in V2-V3, with ST-segment elevations. Relative to the R-waves, T-waves are too big and pointed (differential diagnoses are considered beneath).
Overview of the normal electrocardiogram (ECG)
ECG interpretation includes an assessment of the morphology (appearance) of the waves and intervals on the ECG bend. Therefore, ECG estimation requires a structured cess of the waves and intervals. Before discussing each component in particular, a cursory overview of the waves and intervals is given.
The P-wave, PR interval and PR segment
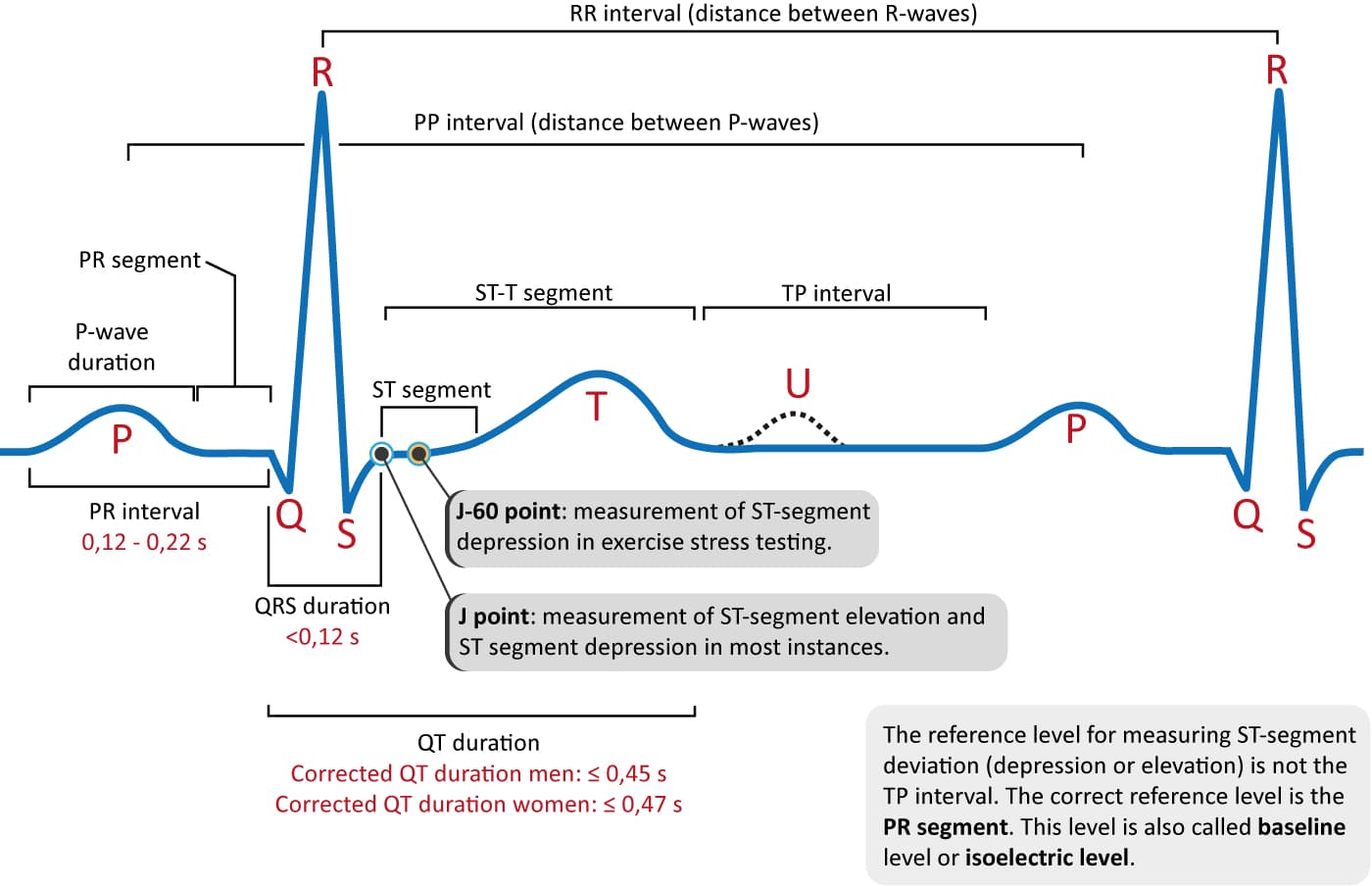
ECG interpretation traditionally starts with an assessment of the P-wave. The P-wave reflects atrial depolarization (activation). The PR interval is the distance between the onset of the P-moving ridge to the onset of the QRS complex. The PR interval is assessed in club to determine whether impulse conduction from the atria to the ventricles is normal. The flat line between the terminate of the P-moving ridge and the onset of the QRS complex is chosen the PR segment and information technology reflects the slow impulse conduction through the atrioventricular node. The PR segment serves as the baseline (besides referred to as reference line or isoelectric line) of the ECG bend. The amplitude of whatsoever deflection/moving ridge is measured past using the PR segment as the baseline. Refer to Effigy 1.
The QRS circuitous
The QRS complex represents the depolarization (activation) of the ventricles. It is always referred to as the "QRS complex" although it may non always brandish all three waves. Since the electrical vector generated by the left ventricle is many times larger than the vector generated by the correct ventricle, the QRS complex is actually a reflection of left ventricular depolarization. QRS duration is the fourth dimension interval from the onset to the end of the QRS complex. A short QRS complex is desirable as it proves that the ventricles are depolarized rapidly, which in plough implies that the conduction system functions properly. Wide (also referred to as broad) QRS complexes bespeak that ventricular depolarization is slow, which may be due to dysfunction in the conduction arrangement.
The J point and the ST segment
The ST segment corresponds to the plateau stage (phase ii) of the action potential. The ST segment must always be studied advisedly since information technology is altered in a wide range of conditions. Many of these atmospheric condition cause rather characteristic ST segment changes. The ST segment is of item interest in the setting of astute myocardial ischemia because ischemia causes deviation of the ST segment (ST segment deviation). There are two types of ST segment deviations. ST segment depression implies that the ST segment is displaced, such that it is below the level of the PR segment. ST segment top implies that the ST segment is displaced, such that information technology is above the level of the PR segment. The magnitude of low/pinnacle is measured every bit the meridian difference (in millimeters) between the J point and the PR segment. The J point is the point where the ST segment starts. If the baseline (PR segment) is difficult to discern, the TP interval may exist used as the reference level.
The T-wave
The T-wave reflects the rapid repolarization of contractile cells (phase iii) and T-moving ridge changes occur in a wide range of weather. T-wave changes are frequently misunderstood in clinical exercise, which the discussion below will endeavour to cure. The transition from the ST segment to the T-wave should be smooth (and non sharp). The normal T-wave is slightly asymmetric, with a steeper downward slope.
The U-wave
The U-wave is seen occasionally. It is a positive moving ridge occurring afterwards the T-wave. Its amplitude is mostly 1-fourth of the T-wave's amplitude. The U-wave is near frequently seen in leads V2–V4. Individuals with prominent T-waves, as well as those with slow center rates, display U-waves more than often. The genesis of the U-moving ridge remains elusive.
QT duration and QTc elapsing
QT elapsing reflects the total duration of ventricular depolarization and repolarization. It is measured from the onset of the QRS complex to the end of the T-wave. The QT duration is inversely related to heart rate; i.east the QT interval increases at slower centre rates and decreases at higher heart rates. Therefore to determine whether the QT interval is inside normal limits, it is necessary to adapt for the heart rate. The center rate-adjusted QT interval is referred to as the corrected QT interval (QTc interval). A long QTc interval increases the risk of ventricular arrhythmias.
Now follows the detailed give-and-take of each ECG of these components.
The P-moving ridge
ECG interpretation ordinarily starts with an assessment of the P-moving ridge. The P-wave is a small, positive and smooth wave. It is modest because the atria make a relatively small muscle mass. If the rhythm is sinus rhythm (i.east nether normal circumstances) the P-wave vector is directed downwards and to the left in the frontal plane and this yields a positive P-wave in lead II (Figure 2, correct-hand side). The P-wave is always positive in lead Ii during sinus rhythm. This is rather easy to sympathize considering lead II is angled alongside the P-wave vector, and the exploring electrode is located in front of the P-moving ridge vector (Figure two, right-hand side).
The P-wave vector is slightly curved in the horizontal airplane. Information technology is initially directed forward but then turns left to activate the left atrium (Figure 2, left-hand side). Lead V1 might therefore brandish a biphasic (diphasic) P-wave, meaning that the greater portion of the P-moving ridge is positive only the terminal portion is slightly negative (the vector generated by left atrial activation heads away from V1). Occasionally, the negative deflection is also seen in lead V2. lead V5 only notes vectors heading towards the exploring electrode (admitting with somewhat varying angles) and therefore displays a positive P-wave throughout.

Figure 2 (above) does not show that the P-wave in lead 2 might actually exist slightly asymmetric by having 2 humps. This is oft (but non e'er) seen on ordinary ECG tracings and it is explained by the fact that the atria are depolarized sequentially, with the right atrium being depolarized before the left atrium. The commencement half of the P-wave is therefore a reflection of right atrial depolarization and the 2d half is a reflection of left atrial depolarization. This is shown in Figure 3 (upper panel). Recall that the P-wave in V1 is oft biphasic, which is also shown in Figure 3.
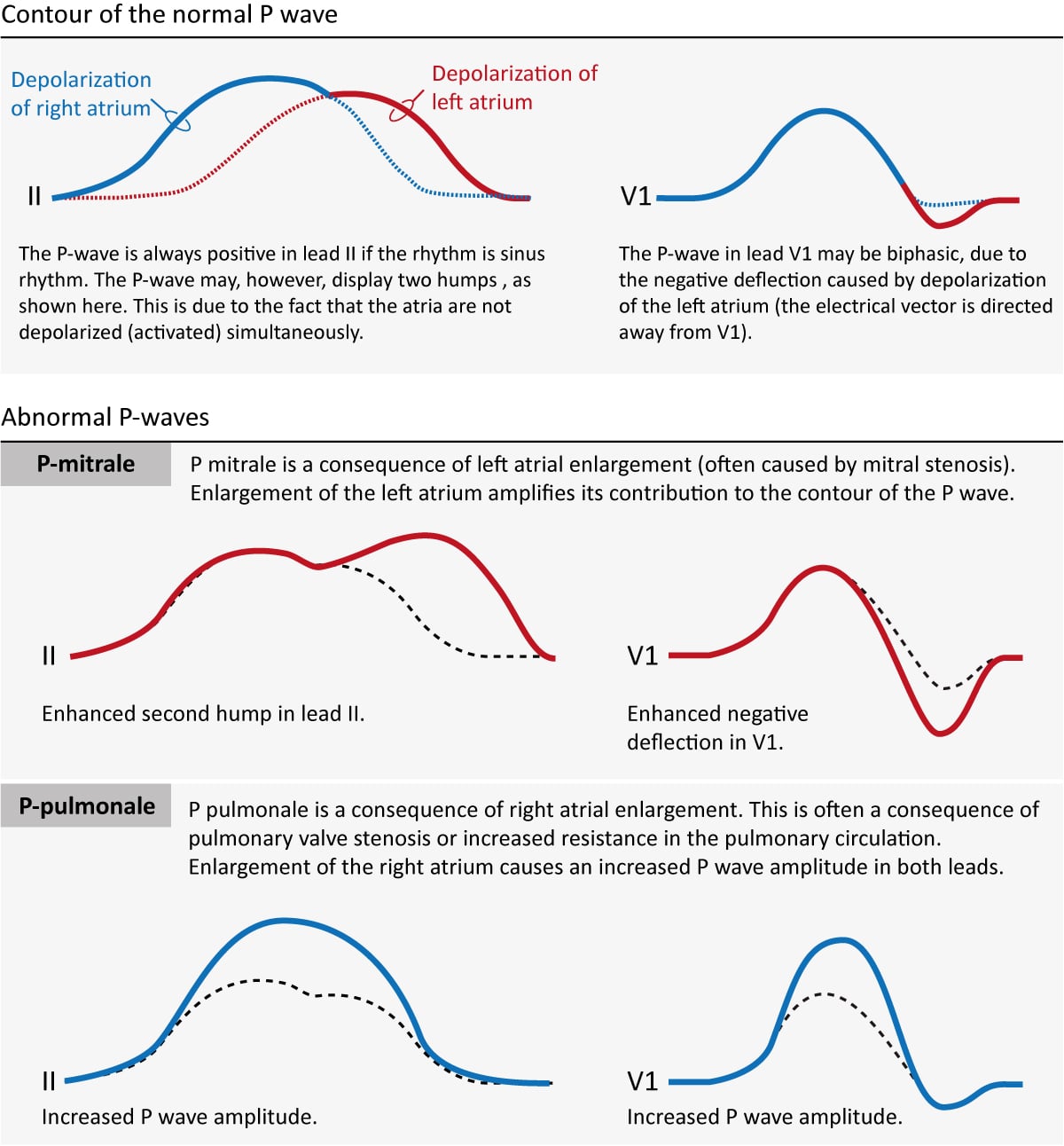
If an atrium becomes enlarged (typically as a compensatory machinery) its contribution to the P-moving ridge will be enhanced. Enlargement of the left and right atria causes typical P-wave changes in pb II and atomic number 82 V1 (Figure 3).
Enlargement of the right atrium is commonly a upshot of increased resistance to empty blood into the right ventricle. This may be due to pulmonary valve stenosis, increased pulmonary avenue pressure etc. The right atrium must then enlarge (hypertrophy) in gild to manage to pump blood into the right ventricle. Right atrial enlargement (hypertrophy) leads to stronger electrical currents and thus enhancement of the contribution of the right atrium to the P-moving ridge. The P-wave volition display higher aamplitude in lead II and lead V1. Such a P-wave is chosen P pulmonale because pulmonary diseases are the nigh mutual causes (Effigy 3, P-pulmonale).
If the left atrium encounters increased resistance (e.g due to mitral valve stenosis) it becomes enlarged (hypertrophy) which amplifies its contribution to the P-wave. The second hump in lead Ii becomes larger and the negative deflection in V1 becomes deeper. This is called P mitrale, because mitral valve affliction is a common crusade (Effigy 25, P-mitrale).
If the atria are depolarized by impulses generated by cells exterior of the sinoatrial node (i.due east by an ectopic focus), the morphology of the P-wave may differ from the P-waves in sinus rhythm. If the ectopic focus is located close to the sinoatrial node, the P-moving ridge volition take a morphology similar to the P-wave in sinus rhythm. Notwithstanding, an ectopic focus may be located anywhere. If it is located near the atrioventricular node, the activation of the atria will proceed in the opposite management, which produces an inverted (retrograde) P-moving ridge.
P-wave checklist
- The P-moving ridge is always positive in pb 2 during sinus rhythm.
- The P-wave is most always positive in leads aVL, aVF, –aVR, I, V4, V5 and V6. It is negative in atomic number 82 aVR.
- The P-wave is oft biphasic in V1 (occasionally in V2). The negative deflection is normally <1 mm.
- P-wave duration should be ≤0,12 seconds.
- P-wave aamplitude should be <2,5 mm in the limb leads.
- P-pulmonale implies that the P-moving ridge has an abnormally high aamplitude in lead II (and in other leads in general).
- P-mitrale implies that the 2nd hump of the P-wave in lead Ii and the negative deflection of the P-wave in lead V1 are both enhanced.
PR interval and PR segment
The PR interval starts at the onset of the P-wave and ends at the onset of the QRS complex (Figure one). Information technology reflects the time interval from the start of atrial depolarization to the start of ventricular depolarization. The PR interval is assessed in society to make up one's mind whether impulse conduction from the atria to the ventricles is normal in terms of speed. The PR interval must not be too long nor as well short. A normal PR interval ranges betwixt 0.12 seconds to 0.22 seconds.
The flat line between the terminate of the P-wave and the onset of the QRS complex is chosen the PR segment and information technology reflects the tedious impulse conduction through the atrioventricular node. The PR segment serves as the baseline (as well referred to every bit reference line or isoelectric line) of the ECG bend. The aamplitude of whatsoever deflection/moving ridge is measured by using the PR segment as the baseline.
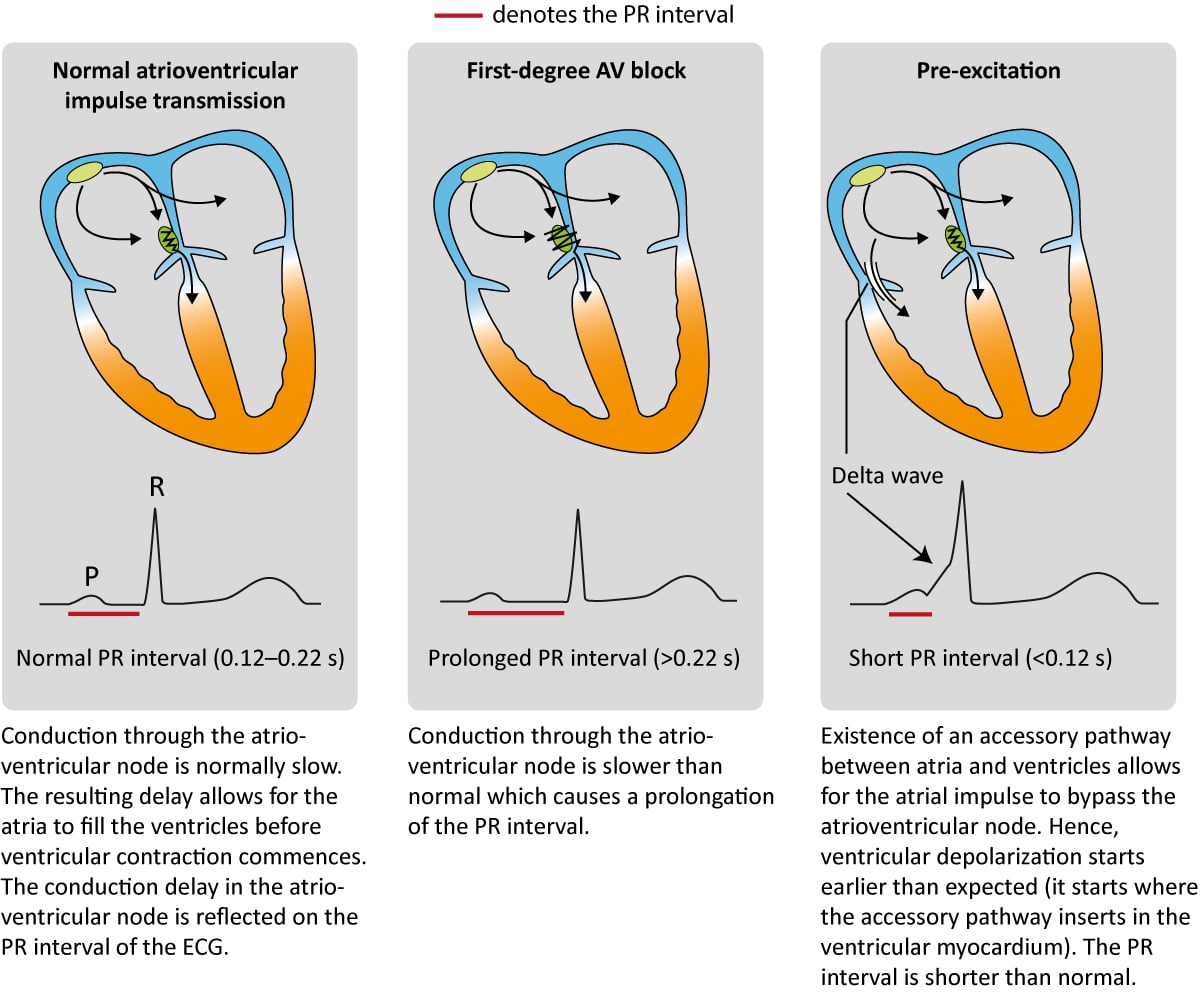
Numerous conditions tin diminish the capacity of the atrioventricular node to conduct the atrial impulse to the ventricles. As the conduction diminishes, the PR interval becomes longer. When the PR interval exceeds 0.22 seconds, first-degree AV-block is manifest. The term block is somewhat misleading since information technology is actually a affair of aberrant delay and not a block per se. The most common cause of outset-degree AV-block is degenerative (age-related) fibrosis in the conduction system. Myocardial ischemia/infarction and medications (eastward.1000 beta-blockers) may also crusade beginning-degree AV-block. Note that the upper reference limit (0.22 seconds) should be related to the historic period of the patient; 0.20 seconds is more than suitable for immature adults because they have faster impulse conduction. Refer to Figure 4 (2nd console). AV-blocks are discussed in item later.
The atrioventricular (AV) node is normally the only connectedness between the atria and the ventricles. The atria and the ventricles are electrically isolated from each other by the fibrous rings (anulus fibrosus). However, information technology is not rare to accept an additional – accompaniment – pathway between the atria and the ventricles. Such an accessory pathway is an embryological remnant that may be located nigh anywhere between the atria and the ventricles. It enables the atrial impulse to pass directly to the ventricles and start ventricular depolarization prematurely. If the atrial impulse uses an accompaniment pathway, the impulse delay in the atrioventricular node is bypassed and therefore the PR interval becomes shortened (PR interval <0.12 seconds). The condition is referred to as pre-excitation because the ventricles are excited prematurely. This is illustrated in Figure 4 (third panel). As seen in Figure 4 (tertiary console) the initial depolarization of the ventricles (starting where the accompaniment pathway inserts into the ventricular myocardium) is tiresome because the impulse will not spread via the normal His-Purkinje pathway. The ho-hum initial depolarization is seen as a delta wave on the ECG (Figure 4, tertiary console). However, apart from the delta moving ridge, the R-wave volition appear normal because ventricular depolarization will be executed normally as soon as the atrioventricular node delivers the impulse to the His-Purkinje system.
PR interval checklist
- Normal PR interval: 0,12–0,22 seconds. The upper reference limit is 0,20 seconds in young adults.
- A prolonged PR interval (>0.22 due south) is consistent with first-caste AV-block.
- A shortened PR interval (<0,12 s) indicates pre-excitation (presence of an accessory pathway). This is associated with a delta wave.
The QRS complex (ventricular complex)
A complete QRS complex consists of a Q-, R- and Southward-wave. Even so, all three waves may non be visible and there is ever variation between the leads. Some leads may display all waves, whereas others might only brandish one of the waves. Regardless of which waves are visible, the wave(s) that reverberate ventricular depolarization is always referred to equally the QRS complex.
Naming of the waves in the QRS circuitous:
The naming of the waves in the QRS circuitous is easy but often misunderstood. The post-obit rules apply when naming the waves:
- A deflection is but referred to every bit a wave if information technology passes the baseline.
- If the first wave is negative then it is referred to as Q-wave. If the first wave is not negative, then the QRS complex does not possess a Q-moving ridge, regardless of the appearance of the QRS circuitous.
- All positive waves are referred to equally R-waves. The showtime positive wave is simply an "R-wave" (R). The 2nd positive wave is called "R-prime wave" (R'). If a third positive wave occurs (rare) information technology is referred to equally "R-bis wave" (R").
- Whatever negative wave occurring after a positive wave is an Due south-moving ridge.
- Large waves are referred to past their capital messages (Q, R, South), and small waves are referred to by their lower-case letters (q, r, southward).
Figure 5 shows examples of the naming of the QRS-complex.

Cyberspace direction of the QRS complex
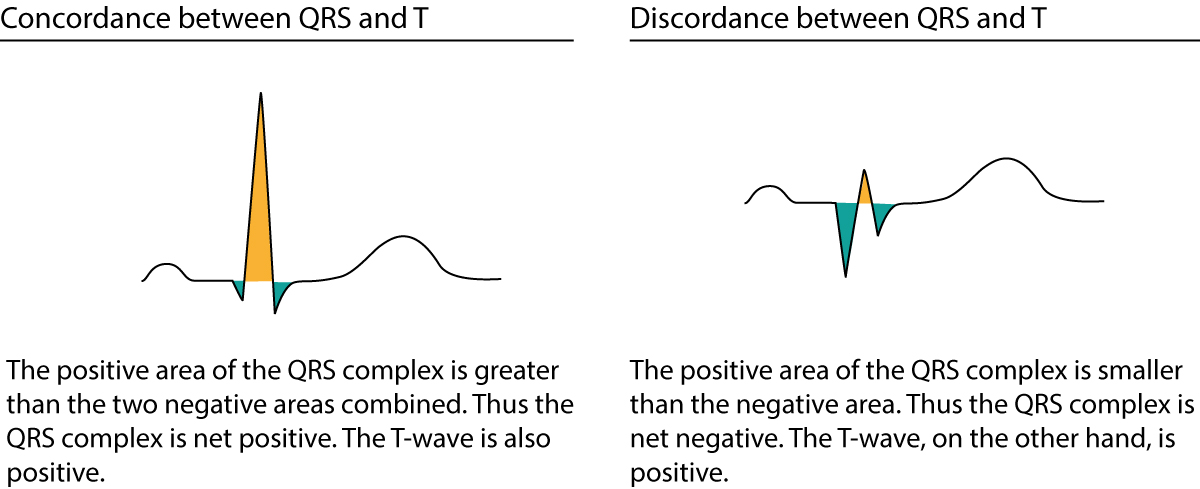
The QRS complex can be classified as net positive or net negative, referring to its cyberspace direction. The QRS complex is net positive if the sum of the positive areas (higher up baseline) exceeds that of the negative areas (below baseline). Refer to Figure 6, console A. These calculations are approximated simply by eyeballing. Panel B in Effigy six shows a net negative QRS circuitous because the negative areas are greater than the positive surface area.

Electric vectors that engender the QRS circuitous
Depolarization of the ventricles generates three large vectors, which explains why the QRS circuitous is composed of three waves. Information technology is key to sympathize the genesis of these waves and although it has been discussed previously a brief rehearsal is warranted. Effigy 7 illustrates the vectors in the horizontal plane. Study Figure 7 carefully, as it illustrates how the P-wave and QRS complex are generated by the electric vectors.

Notation that the commencement vector in Effigy 7 is not discussed hither as information technology belongs to atrial activity.
The second vector: the ventricular (interventricular) septum
The ventricular septum receives Purkinje fibers from the left packet branch and therefore depolarization proceeds from its left side towards its correct side. The vector is directed frontward and to the right. The ventricular septum is relatively small, which is why V1 displays a pocket-sized positive moving ridge (r-wave) and V5 displays a small negative wave (q-wave). Thus, it is the aforementioned electrical vector that results in an r-wave in V1 and q-wave in V5.
The tertiary vector: the ventricular free wall
The vectors resulting from activation of the ventricular free walls are directed to the left and downwards (Effigy 7). The explanation for this is as follows:
- The vector resulting from activation of the right ventricle does not come to expression, considering it is drowned by the many times larger vector generated by the left ventricle. Thus, the vector during activation of the ventricular free walls is really the vector generated by the left ventricle.
- Activation of the ventricular gratis wall proceeds from the endocardium to the epicardium. This is because the Purkinje fibers run through the endocardium, where they deliver the action potential to contractile cells. The subsequent spread of the activeness potential occurs from one contractile cell to some other, starting in the endocardium and heading towards the epicardium.
Equally axiomatic from Figure 7, the vector of the ventricular free wall is directed to the left (and downward). Lead V5 detects a very large vector heading towards it and therefore displays a large R-wave. Lead V1 records the opposite and therefore displays a large negative moving ridge called S-wave.
The quaternary vector: basal parts of the ventricles
The concluding vector stems from the activation of the basal parts of the ventricles. The vector is directed backward and up. Information technology heads away from V5 which records a negative wave (s-wave). Pb V1 does non find this vector.
Implications and causes of broad (broad) QRS complex
Prolongation of QRS elapsing implies that ventricular depolarization is slower than normal. The QRS duration is generally <0,10 seconds but must be <0,12 seconds. If QRS elapsing is ≥ 0,12 seconds (120 milliseconds) then the QRS circuitous is abnormally wide (broad). This is very common and a significant finding. The reason for wide QRS complexes must always be clarified. Clinicians often perceive this equally a difficult chore despite the fact that the list of differential diagnoses is rather short. The following causes of wide QRS complexes must be familiar to all clinicians:
- Bundle branch cake: The left and the right package branch consists of Purkinje fibers which spread out into the ventricular myocardium. The Purkinje network enables fast impulse conduction and then that the action potential can be delivered to the whole myocardium at the same time (approximately). A package branch block occurs if a bundle branch is dysfunctional and unable to transmit the impulse. The ventricle whose package is blocked will take to wait for electric impulses to spread from the other ventricle. Considering the spread of the impulse from the other ventricle volition take identify partly or entirely exterior of the conduction system, it will be slow and therefore the QRS duration is prolonged. Left and right parcel branch cake are discussed in separate manufactures.
- Hyperkalemia: Hyperkalemia causes tiresome impulse transmission (in all myocardial and conduction cells) and prolongation of the QRS duration.
- Drugs: form I antiarrhythmic drugs, tricyclic antidepressants, and other medications can cause widening of the QRS circuitous.
- Ventricular rhythm, ventricular ectopy, and pacemaker with ventricular stimulation:
- Spontaneous action potentials discharged within the ventricles may depolarize the ventricles. The cell/structure which discharges the action potential is referred to as an ectopic focus. Such a focus may fire single or multiple impulses (either consecutively or intermittently). A single impulse gives rising to a premature ventricular vanquish, whereas multiple impulses may plant a ventricular rhythm, or even ventricular tachycardia. In all these instances the QRS complex will be broad because the depolarizing impulse arises and spreads outside of the normal conduction system.
- External (artificial) pacemakers have an electrode inserted in the correct ventricular apex. Electrical stimulation in the right ventricular apex will give rise to an action potential propagating from in that location, i.eastward partly or entirely exterior of the conduction system (which will crusade broad QRS complexes).
- Pre-excitation (Wolff-Parkinson-White syndrome): Pre-excitation implies the beingness of an accessory pathway (in addition to the atrioventricular node) between the atria and the ventricles. Such pathways virtually always insert into the ventricular myocardium, from where the action potential spreads. Again, the spread takes place outside of the conduction arrangement which is slow and causes widening of the QRS circuitous.
- Aberrant ventricular conduction (aberrancy): Aberrant conduction is really a bundle co-operative block that occurs when the length of the cardiac cycle is speedily inverse, particularly at high centre rates. The bundle branches (particularly the right bundle co-operative) may occasionally fail to adapt their repolarization menstruation to the length of the cardiac bike (which they also do). This is discussed in detail in the article on abnormal ventricular conduction.
Figure 8 (below) shows examples of normal and abnormally broad QRS complexes at 25 mm/s and l mm/s paper speed.

Amplitude of the QRS complex
A QRS complex with large amplitudes may be explained by ventricular hypertrophy or enlargement (or a combination of both). The electrical currents generated by the ventricular myocardium are proportional to the ventricular musculus mass. Hypertrophy ways that there are more than muscles and hence larger electric potentials generated. Withal, the distance between the heart and the electrodes may take a pregnant bear upon on the amplitudes of the QRS complex. For example, slender individuals by and large have a shorter distance between the heart and the electrodes, as compared with obese individuals. Therefore, the slender private may nowadays with much larger QRS amplitudes. Similarly, a person with chronic obstructive pulmonary disease (COPD) frequently displays diminished QRS amplitudes due to hyperinflation of the thorax (increased altitude to electrodes). Low amplitudes may also be caused by hypothyreosis. In the setting of circulatory collapse, low amplitudes should raise suspicion of cardiac tamponade.
R-wave amplitude
It is of import to assess the aamplitude of the R-waves. Loftier amplitudes may be due to ventricular enlargement or hypertrophy. To make up one's mind whether the amplitudes are enlarged, the post-obit references are at paw:
- R-wave should be < 26 mm in V5 and V6.
- R-wave amplitude in V5 + Southward-wave amplitude in V1 should be <35 mm.
- R-wave amplitude in V6 + Southward-wave amplitude in V1 should be <35 mm.
- R-wave aamplitude in aVL should be ≤ 12 mm.
- R-moving ridge amplitude in leads I, 2 and III should all be ≤ 20 mm.
- If R-wave in V1 is larger than S-wave in V1, the R-wave should be <5 mm.
(1 mm corresponds to 0.1 mV on standard ECG grid).
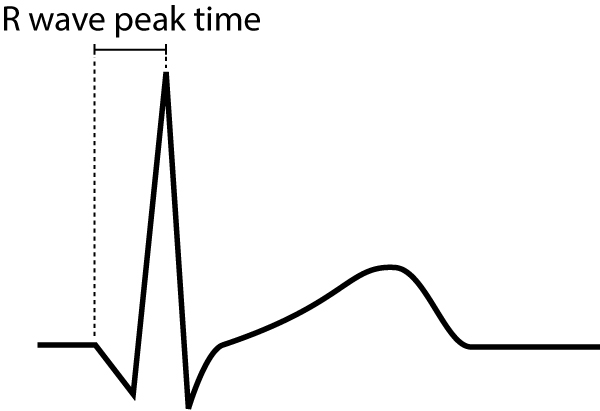
R-wave peak time
R-wave peak time (Figure 9) is the interval from the starting time of the QRS-circuitous to the apex of the R-wave. This interval reflects the time elapsed for the depolarization to spread from the endocardium to the epicardium. R-moving ridge peak time is prolonged in hypertrophy and conduction disturbances.
Normal values for R-moving ridge elevation time follow:
- Leads V1-V2 (right ventricle) <0,035 seconds
- Leads V5-V6 (left ventricle) <0,045 seconds
R-moving ridge progression
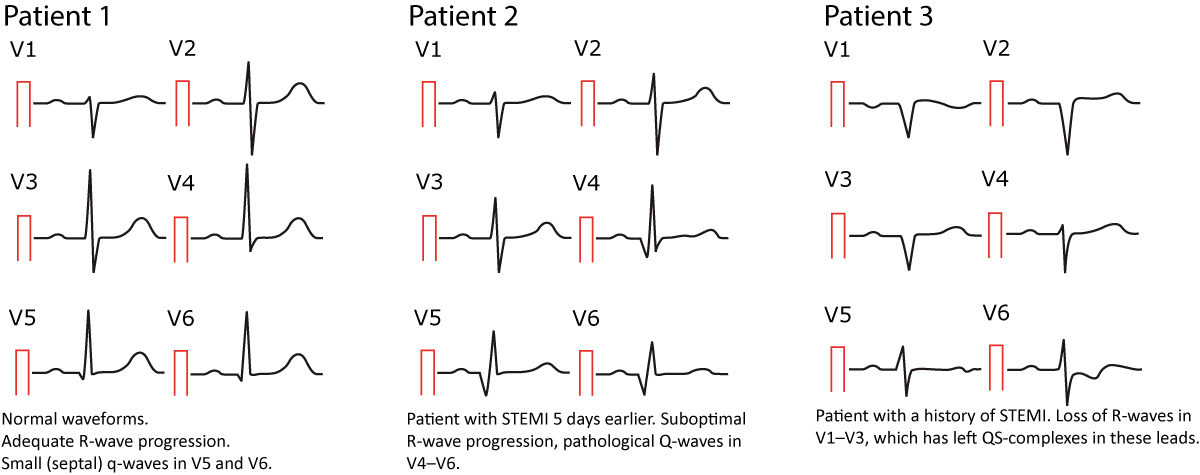
R-wave progression is assessed in the chest (precordial) leads. Normal R-moving ridge progression implies that the R-wave gradually increases in amplitude from V1 to V5 and so diminishes in amplitude from V5 to V6 (Effigy 10, left-hand side). The Southward-wave undergoes the opposite development. Abnormal R-wave progression is a common finding which may be explained past any of the following conditions:
- Myocardial infarction: necrotic myocardium does not generate electrical potentials and therefore there is a loss of R-wave amplitude in the ECG leads reflecting the necrotic area (Figure 10, right-hand side).
- Cardiomyopathy may cause either loss or proceeds of R-wave amplitude, depending on the type of cardiomyopathy. Amplitudes may be increased in hypertrophic cardiomyopathy, whereas they are typically diminished in late stages of dilated cardiomyopathy.
- Right and left ventricular hypertrophy as well amplifies the R-moving ridge amplitude. Left ventricular hypertrophy causes increased R-moving ridge amplitudes in V4–V6 and deeper Southward-waves in V1–V3. Correct ventricular hypertrophy causes large R-waves in V1–V3 and smaller R-waves in V4–V6.
- Pre-excitation, bundle co-operative block and chronic obstructive pulmonary disease (COPD) may also impact R-wave progression. These conditions are discussed in detail later on.
Annotation that the R-moving ridge is occasionally missing in V1 (may exist due to misplacement of the electrode). This is considered a normal finding provided that an R-wave is seen in V2.

Dominant R-wave in V1/V2
As seen in Figure 10 (left-hand side) the R-moving ridge in V1–V2 is considerably smaller than the S-wave in V1–V2. Dominant R-wave in V1/V2 implies that the R-wave is larger than the S-wave, and this may exist pathological. If the R-wave is larger than the S-moving ridge, the R-wave should be <five mm, otherwise the R-wave is abnormally large. This may exist explained by right bundle branch cake, right ventricular hypertrophy, hypertrophic cardiomyopathy, posterolateral ischemia/infarction (if the patient experiences chest pain), pre-excitation, dextrocardia or misplacement of chest electrodes.
The Q-wave
It is crucial to differentiate normal from pathological Q-waves, particularly because pathological Q-waves are rather firm evidence of previous myocardial infarction. All the same, there are numerous other causes of Q-waves, both normal and pathological and it is of import to differentiate these.
The amplitude (depth) and the duration (width) of the Q-wave dictate whether it is aberrant or non. Pathological Q-waves have a duration ≥0,03 sec and/or amplitude ≥25% of the R-wave aamplitude. Pathological Q-waves must exist in at to the lowest degree two anatomically contiguous leads (i.e neighboring leads, such as aVF and Three, or V4 and V5) in social club to reflect an actual morphological abnormality. The existence of pathological Q-waves in two contiguous leads is sufficient for a diagnosis of Q-wave infarction. This is illustrated in Figure 11.

Normal variants of Q-waves
Septal q-waves are pocket-sized q-waves oftentimes seen in the lateral leads (V5, V6, aVL, I). They are due to the normal depolarization of the ventricular septum (see the previous discussion). Two minor septal q-waves can really be seen in V5–V6 in Figure x (left-hand side).
An isolated and often large Q-wave is occasionally seen in lead III. The amplitude of this Q-wave typically varies with ventilation and it is therefore referred to equally a respiratory Q-moving ridge. Notation that the Q-wave must be isolated to lead Iii (i.east the neighboring atomic number 82, which is aVF, must non display a pathological Q-moving ridge).
As noted above, the small r-wave in V1 is occasionally missing, which leaves a QS-complex in V1 (a QRS complex consisting of just a Q-moving ridge is referred to as a QS-complex). This is considered a normal finding provided that pb V2 shows an r-moving ridge. If the R-wave is missing in atomic number 82 V2 equally well, then the criteria for pathology is fulfilled (ii QS-complexes).
Small Q-waves (which do non fulfill criteria for pathology) may be seen in all limb leads as well as V4–V6. If these Q-waves do not fulfill the criteria for pathology, then they should be accustomed. Leads V1–V3, on the other paw, should never display Q-waves (regardless of their size).
Abnormal (pathological) Q-waves
The most common cause of pathological Q-waves is myocardial infarction. If myocardial infarction leaves pathological Q-waves, it is referred to every bit Q-wave infarction. Criteria for such Q-waves are presented in Figure 11. Note that pathological Q-waves must exist in 2 anatomically contiguous leads.
Other causes of abnormal Q-waves are as follows:
- Left-sided pneumothorax
- Dextrocardia
- Perimyocarditis
- Cardiomyopathy
- Amyloidosis
- Bundle branch blocks, fascicular blocks
- Pre-excitation (WPW syndrome)
- Ventricular hypertrophy
- Acute cor pulmonale
To differentiate these causes of abnormal Q-waves from Q-wave infarction, the following can exist advised:
- If it is unlikely that the patient has coronary heart disease, other causes are more likely. It should exist noted, however, that up to 20% of Q-moving ridge infarctions may develop without symptoms (The Framingham Heart Study).
- If coronary heart disease is likely, then infarction is the virtually likely cause of the Q-waves.
- The longer the Q-wave elapsing, the more probable it is that infarction is the cause of the Q-waves. Infarction Q-waves are typically >40 ms.
Examples of normal and pathological Q-waves (later on acute myocardial infarction) are presented in Figure 12 beneath.
The ST segment: ST low & ST elevation
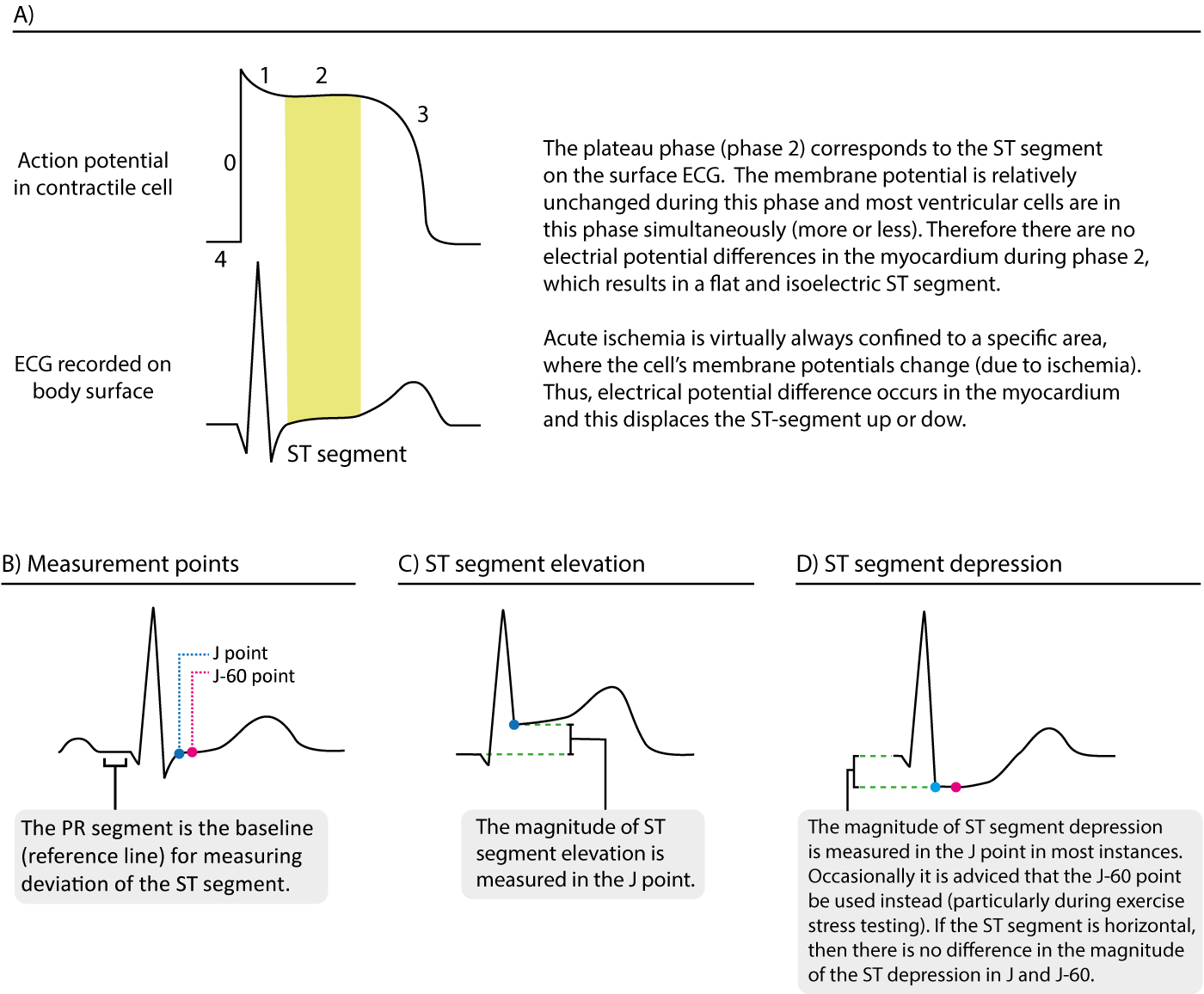
The ST segment corresponds to the plateau stage of the action potential (Effigy 13). The ST segment extends from the J betoken to the onset of the T-moving ridge. Because of the long elapsing of the plateau phase virtually contractile cells are in this phase at the aforementioned time (more or less). Moreover, the membrane potential is relatively unchanged during the plateau phase. These two factors are the reason why the ST segment is flat and isoelectric (i.e in level with the baseline).
Deportation of the ST segment is of key importance, particularly in acute myocardial ischemia. Considering myocardial ischemia affects a limited area and disturbs the cells' membrane potential (during phase 2), it engenders an electrical potential difference in the myocardium. The electrical potential difference exists betwixt ischemic and normal myocardium and information technology results in the displacement of the ST segment. The ST segment may be displaced upwards (ST segment elevation) or downwards (ST segment low). The term ST segment divergence refers to tiptop and depression of the ST segment. The magnitude of ST segment difference is measured as the height difference (in millimeters) between the J point and the PR segment. Refer to Effigy 13 for examples.
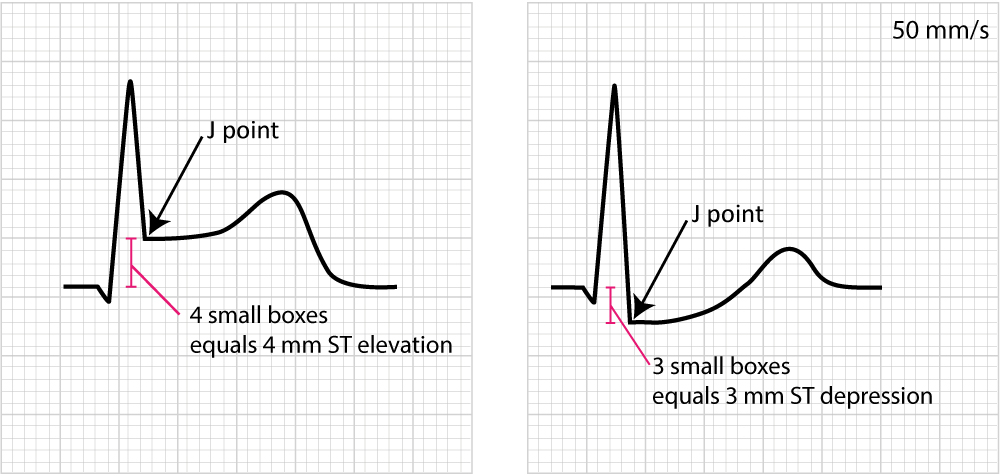
Figure 14 below shows how to measure out ST segment deviation.
The post-obit must be noted regarding the ST segment:
- The normal ST segment is flat and isoelectric. The transition from ST segment to T-wave is smoothen, and not abrupt.
- ST segment deviation (elevation, depression) is measured as the height difference (in millimeters) between the J bespeak and the baseline (the PR segment). ST segment deviation occurs in a wide range of weather condition, especially acute myocardial ischemia.
- Because the ST segment and the T-wave are electrophysiologically related, changes in the ST segment are frequently accompanied by T-wave changes. The term ST-T segment changes (or simply ST-T changes) is used to refer to such ECG changes.
It must also be noted that the J point is occasionally suboptimal for measuring ST segment departure. This is explained past the fact that the J point is not always isoelectric; this occurs if there are electric potential differences in the myocardium past the end of the QRS complex (information technology typically causes J point depression). The reason for such electrical potential difference is that not all ventricular myocardial cells will stop their action potential simultaneously. Myocardial cells which depolarized at the beginning of the QRS complex will not be in the exact same stage as cells that depolarized during the end of the QRS complex. Due to this, it is sometimes recommended that ST segment deviation be measured in the J-sixty point, or J-fourscore point, which is located sixty and 80 milliseconds, respectively, after the J point (Comprehensive Electrocardiology, MacFarlane et al, Springer, 2010; Chou'due south Electrocardiologi, Surawicz, Elsevier 2010). At the fourth dimension of J-60 and J-lxxx, there is minimal chance that there are any electrical potential differences in the myocardium. Current guidelines, however, still recommend the utilise of the J bespeak for assessing astute ischemia (Third Universal Definition of Myocardial Infarction, Thygesen et al, Circulation). A notable exception to this rule is the practice stress test, in which the J-sixty or J-eighty is always used (because practice ofttimes causes J point depression).
As mentioned to a higher place at that place are numerous other conditions that touch on the ST-T segment and it is fundamental to be able to differentiate these. For this purpose, it is wise to subdivide ST-T changes into primary and secondary.
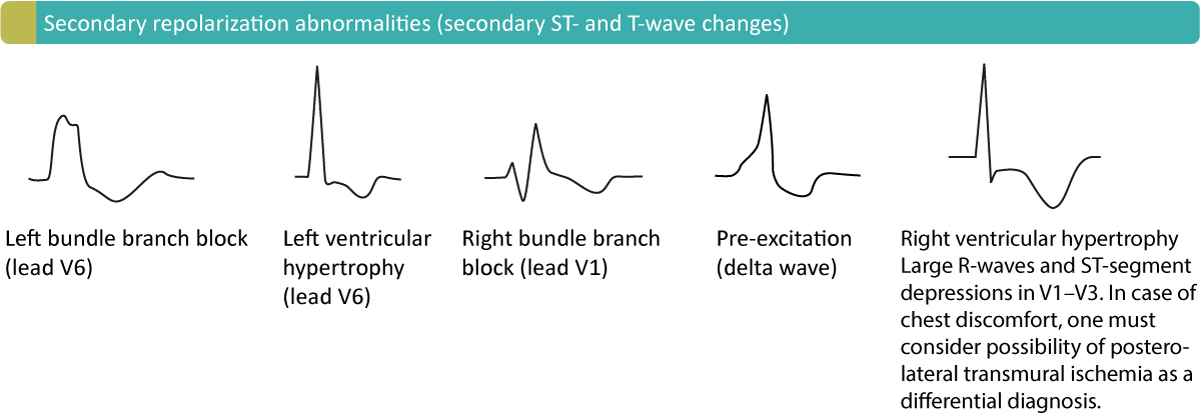
Principal and secondary ST-T changes
Primary ST-T changes are caused by abnormal repolarization. This is seen in ischemia, electrolyte disorders (calcium, potassium), tachycardia, increased sympathetic tone, drug side effects etc.
Secondary ST-T changes occur when abnormal depolarization causes abnormal repolarization. This is seen in bundle branch blocks (left and right package branch block), pre-excitation, ventricular hypertrophy, premature ventricular complexes, pacemaker stimulated beats etc. In each of these weather condition, the depolarization is abnormal and this affects the repolarization so that it cannot be carried out unremarkably.
The next give-and-take will exist devoted to characterizing of import and common ST-T changes.
ST segment low
ST segment depression is measured in the J point. The reference point is, as usual, the PR segment. ST segment depression less than 0.5 mm is accustomed in all leads. ST segment depression 0.5 mm or more is considered pathological. Some expert consensus documents also note that any ST segment depression in V2–V3 should be considered abnormal (considering healthy individuals rarely display depressions in those leads). Delight annotation that every cause of ST segment depression discussed beneath is illustrated in Figure xv. Report this effigy carefully.

Principal ST depressions
Physiological ST segment depressions occur during physical exercise. These ST segment depressions display an upsloping ST segment, typically depressed <one mm in the J-60 indicate and the depressions are normalized quickly after the exercise has concluded. Hyperventilation brings most the aforementioned ST segment depressions as concrete exercise. Figure 15 A.
Digoxin causes generalized ST segment depressions with a curved ST segment (generalized implies that the depression can exist seen in most ECG leads). Figure 15 B.
Sympathetic tone and hypokalemia cause ST segment depressions (typically <0.5 mm).
Heart failure may crusade ST segment depression in the left lateral leads (V5, V6, aVL and I) and these depressions are generally horizontal or downsloping.
Supraventricular tachycardias as well crusade ST segment depressions which typically occur in V4–V6 with a horizontal or slightly upsloping ST segment. These ST segment low should resolve inside minutes afterwards termination of the tachycardia.
Ischemic ST depressions display a horizontal or downsloping ST segment (this is a requirement according to Due north American and European guidelines). The horizontal ST segment low is most typical of ischemia (Effigy 15 C). ST segment depressions with upsloping ST segments are rarely caused by myocardial ischemia. Even so, there is one notable exception, when an upsloping ST segment is really caused past ischemia and the condition is actually alarming. Upsloping ST segment depressions which are accompanied by prominent T-waves in the majority of the precordial leads may be acquired by astute occlusion of the left anterior descending coronary artery (LAD). This constellation – with upsloping ST low and prominent T-waves in the precordial leads during chest discomfort – is referred to equally de Winters sign (Figure 15 C).
Secondary ST depression
Secondary ST segment depressions occur in the post-obit conditions:
- Left ventricular hypertrophy
- Right ventricular hypertrophy
- Left bundle co-operative cake
- Right packet branch block
- Pre-excitation
- Pacemaker stimulation in the (right) ventricle
These are all common conditions in which an abnormal depolarization (altered QRS complex) causes abnormalities in the repolarization (altered ST-T segment). For instance, a block in the left bundle branch means that the left ventricle will not be depolarized via the Purkinje network, only rather via the spread of the depolarization from the right ventricle. The aberrant ventricular depolarization will cause abnormal repolarization. As evident from Effigy 35 (panel D) these atmospheric condition are characterized by oppositely directed QRS- and ST-T-segments (recollect that this is referred to equally discordance). Hence, ECG leads with cyberspace positive QRS complexes will bear witness ST segment depressions (too equally T-moving ridge changes).
ECG changes in myocardial ischemia are discussed in section 3 (Acute & Chronic Myocardial Ischemia & Infarction) and a specific chapter discusses ST depression.
ST segment elevation
ST segment elevation is measured in the J-point. In the setting of breast discomfort (or other symptoms suggestive of myocardial ischemia) ST segment height is an alarming finding as it indicates that the ischemia is extensive and the hazard of malignant arrhythmias is loftier. Nonetheless, there are many other causes of ST segment elevations and for obvious reasons, one must be able to differentiate these. Figure sixteen displays characteristics of ischemic and non-ischemic ST segment elevations. This figure must also be studied in detail.

Ischemia typically causes ST segment elevations with straight or convex ST segments (Figure 16, panel A). The directly ST segment can be either upsloping, horizontal or (rarely) downsloping. Non-ischemic ST segment elevations are typically concave (Figure 16, console B). Concave ST segment elevations are extremely mutual in any population; e.g ST segment superlative in leads V2–V3 occurs in lxx% of all men under the age of 70. There is no definite mode to rule out myocardial ischemia by judging the appearance of the ST segment, which is why North American and European guidelines assert that the appearance of the ST segment cannot be used to rule out ischemia. ECG changes in ischemia are discussed in detail in section three (Acute & Chronic Myocardial Ischemia & Infarction) and a specific chapter discusses ST elevation in detail.
The T-wave
Cess of the T-moving ridge represents a hard but key part of ECG estimation. The normal T-wave in adults is positive in most precordial and limb leads. The T-wave amplitude is highest in V2–V3. The amplitude diminishes with increasing age. Equally noted above, the transition from the ST segment to the T-wave should be shine. The T-wave is normally slightly asymmetric since its downslope (2d half) is steeper than its upslope (first half). Women have a more than symmetrical T-wave, a more distinct transition from ST segment to T-moving ridge and lower T-wave aamplitude.
The T-wave should be concordant with the QRS complex, meaning that a net positive QRS complex should be followed by a positive T-moving ridge, and vice versa (Figure 17). Otherwise, there is discordance (opposite directions of QRS and T) which might be due to pathology. A negative T-wave is also called an inverted T-wave.
T-moving ridge changes are notoriously misinterpreted, especially inverted T-waves. Below follows a discussion which aims to clarify some of the common misunderstandings. All T-waves are illustrated in Figure eighteen.

Positive T-waves
Positive T-waves are rarely higher than 6 mm in the limb leads (typically highest in lead II). In the chest leads the amplitude is highest in V2–V3, where information technology may occasionally reach x mm in men and 8 mm in women. Normally, though, the amplitude in V2–V3 is effectually vi mm and 3 mm in men and women, respectively. T-waves that are higher than 10 mm and 8 mm, in men and women, respectively, should be considered aberrant. A common cause of abnormally large T-waves is hyperkalemia, which results in high, pointed and slightly asymmetric T-waves. These must exist differentiated from hyperacute T-waves seen in the very early on phase of myocardial ischemia. Hyperacute T-waves are broad-based, high and symmetric. Their duration is short; they typically disappear inside minutes after a total occlusion in a coronary artery occurs (so, of course, the ST segment will be elevated).
T-wave inversion (inverted / negative T-waves)
T-wave inversion means that the T-wave is negative. The T-wave is negative if its terminal portion is below the baseline, regardless of whether its other parts are above the baseline. T-wave inversions are frequently misunderstood, specially in the setting of ischemia.
Normal T-moving ridge inversion
An isolated (unmarried) T-wave inversion in lead V1 is mutual and normal. Information technology is mostly concordant with the QRS complex (which is negative in atomic number 82 V1). Isolated T-wave inversions also occur in leads V2, Iii or aVL. In any instance, one must verify whether the inversion is isolated, because if there is T-wave inversion in two anatomically face-to-face leads, then information technology is pathological.
T-moving ridge inversion in myocardial ischemia
Ischemia never causes isolated T-moving ridge inversions. It is a general misunderstanding that T-wave inversions, without simultaneous ST-segment departure, point acute (ongoing) myocardial ischemia. T-wave inversions without simultaneous ST-segment deviation are not ischemic! However, T-moving ridge inversions that are accompanied past ST-segment deviation (either low or summit) is representative of ischemia (but in that scenario, it is actually the ST-segment deviation that signals that the ischemia is ongoing). Then one might wonder why T-wave inversions are included as criteria for myocardial infarction. This is explained past the fact that T-wave inversions do occur after an ischemic episode, and these T-moving ridge inversions are referred to as mail service-ischemic T-waves. Such T-waves are seen after periods of ischemia, afterward infarction and after successful reperfusion (PCI).
Mail-ischemic T-moving ridge inversion is acquired past abnormal repolarization. These T-wave inversions are symmetric with varying depth. They may be gigantic (10 mm or more) or less than 1 mm. Negative U-waves may occur when post-ischemic T-wave inversions are present. T-wave inversions may actually become chronic after myocardial infarction. Normalization of T-wave inversion after myocardial infarction is a adept prognostic indicator. Delight refer to Effigy 37.
Secondary T-wave inversion
Secondary T-wave inversions – similar to secondary ST-segment depressions – are acquired by packet branch block, pre-excitation, hypertrophy, and ventricular pacemaker stimulation. T-wave inversions that are secondary to these conditions are typically symmetric and in that location is simultaneous ST-segment depression. Note that the T-wave inversion may actually persist for a flow afterward the normalization of the depolarization (if it occurs). This is referred to as T-moving ridge memory or cardiac memory. Secondary T-wave inversions are illustrated in Effigy nineteen (likewise as Figure 18 D).
Flat T-waves
T-waves with very low amplitude are common in the mail-ischemic menses. They are commonly seen in leads V1–V3 if the stenosis/occlusion is located in the left inductive descending avenue. If the stenosis/occlusion is located in the left circumflex avenue or right coronary avenue, the apartment T-waves are seen in leads Two, aVF and III.
Biphasic (diphasic) T-waves
A biphasic T-wave has a positive and a negative deflection (Figure 37, panel C). Information technology should be noted that the term "biphasic" is unfortunate because (1) biphasic T-waves behave no particular significance and (2) a T-moving ridge is classified as positive or inverted based on its terminal portion; if the terminal portion is positive so the T-wave is positive and vice versa. Thus, a biphasic T-wave should exist classified accordingly.
The T-waves in children and adolescents
The T-wave vector is directed to the left, downwards and to the back in children and adolescents. This explains why these individuals display T-wave inversions in the chest leads. T-wave inversions may be nowadays in all chest leads. However, these inversions are normalized gradually during puberty. Some individuals may display persisting T-wave inversion in V1–V4, which is chosen persisting juvenile T-wave design. If all T-waves persist inverted into adulthood, the condition is referred to equally idiopathic global T-moving ridge inversion.
T-wave progression
T-moving ridge progression follows the same rules every bit R-wave progression (meet earlier discussion).
T-wave checklist
- I, II, -aVR, V5 and V6: should display positive T-waves in adults. aVR displays a negative T-wave.
- 3 and aVL: These leads occasionally display an isolated (unmarried) T-wave inversion.
- aVF: positive T-wave, but occasionally flat.
- V1: Inverted or flat T-wave is rather common, particularly in women. The inversion is concordant with the QRS circuitous.
- V7–V9: should brandish a positive T-wave.
U-moving ridge
A U-wave is occasionally seen later on the T-wave. It is not known what engenders the U-wave. It is typically most prominent in leads V2–V3. young people, as well as athletes, take more prominent U-waves. Moreover, the U-moving ridge is more prominent during slower centre rates. The height of the U-wave is typically i-third of the T-moving ridge. Its kickoff half is steeper than its second half.
U-wave inversion is rare merely when seen, it is a strong indicator of pathology, particularly for ischemic heart disease and hypertension.
QT duration and corrected QT (QTc) duration
ECG interpretation always includes an assessment of the QT (QTc) duration. The QT duration represents the total fourth dimension for de- and repolarization. It is measured from the beginning of the QRS-complex to the end of the T-wave. Prolonged QT duration predisposes to life-threatening ventricular arrhythmias and therefore QT elapsing must ever exist assessed. Prolonged QT elapsing may either be congenital (genetic mutations, so-chosen long QT syndrome) or caused (medications, electrolyte disorders). QT duration is inversely related to centre rate; QT duration increases at low center rate and vice versa. Therefore i must suit the QT duration for the heart rate, which yield corrected QT elapsing (Qtc). Bazett's formula has traditionally been used to calculate the corrected QT duration. The formula follows (all variables in seconds):
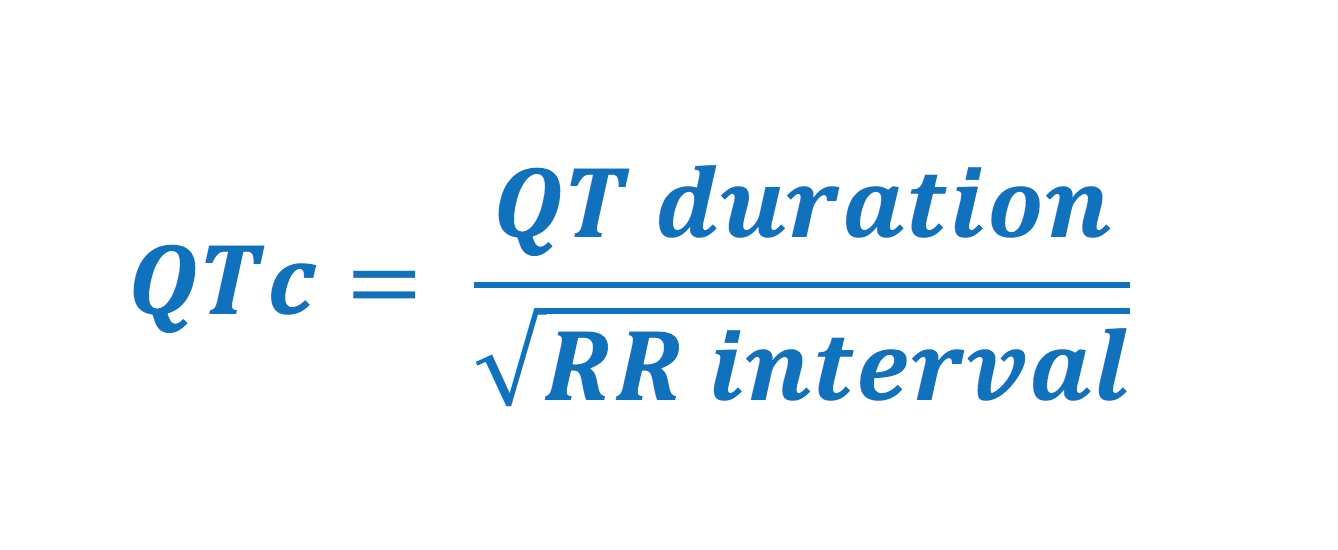
Normal values for QTc interval
- Men: <0,450 seconds
- Women: <0,460 seconds
Nonetheless, Bazett's formula is several decades old and has been questioned because it performs poorly at very low and very high heart rates. Newer formulas (which are incorporated in modern ECG machines) are to be preferred over Bazett's formula. QTc duration is calculated automatically in all modernistic ECG machines. The result is based on the lead with the longest QTc duration (typically leads V2–V3).
Causes of prolonged QTc duration: antiarrhythmics (procainamide, disopyramide, amiodarone, sotalol), psychiatric medications (tricyclic antidepressants, SSRI, lithium etc); antibiotics (macrolides, kinolones, atovaquone, klorokine, amantadine, foscarnet, atazanavir); hypokalemia, hypocalcemia, hypomagnesemia; cerebrovascular insult (bleeding); myocardial ischemia; cardiomyopathy; bradycardia; hypothyroidism; hypothermia. A complete list of drugs causing QT prolongation can be establish here.
Brusk QTc syndrome (QTc <0,390 seconds) is uncommon and can be seen in hypercalcemia and during digoxin handling. It is very rare simply may cause malignant arrhythmias.
QT dispersion
The QT interval varies somewhat in the different leads. The departure betwixt the shortest and the longest QT interval is the QT dispersion. Increased QT dispersion is associated with increased morbidity and mortality. This is presumably explained by a college incidence of cancerous ventricular arrhythmias. It has been suggested that the high risk of ventricular arrhythmias is due to the vulnerability caused by marked local differences in the repolarization.
The electrical axis of the heart (centre axis)
Although often ignored, assessment of the electric axis is an integral part of ECG interpretation. The electrical axis reflects the boilerplate management of ventricular depolarization during ventricular contraction. The management of the depolarization (and thus the electric centrality) is generally aslope the hearts longitudinal axis (to the left and downwards). Figure 38 shows the coordinate system where the green surface area displays the range of normal heart axis.
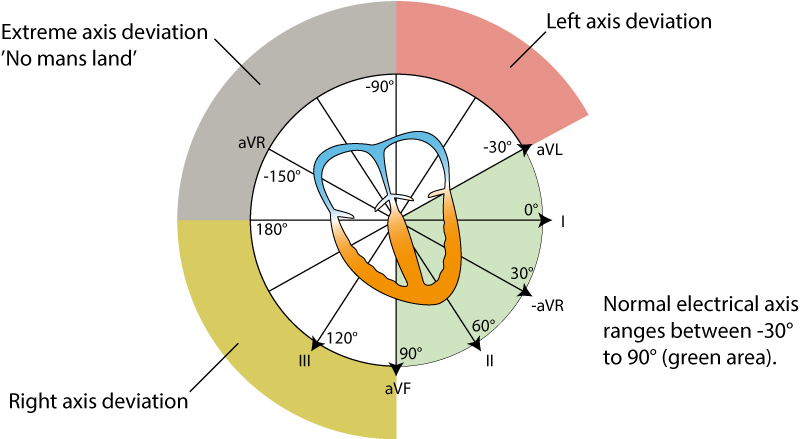
As evident from the effigy, the normal heart axis is between –30° and xc°. If the axis is more positive than xc° it is referred to as right axis deviation. If the centrality is more negative than –xxx° it is referred to as left axis deviation. The centrality is calculated (to the nearest degree) by the ECG machine. The axis can likewise exist approximated manually by judging the net direction of the QRS complex in leads I and II. The following rules use:
- Normal axis: Net positive QRS circuitous in leads I and II.
- Correct axis deviation: Net negative QRS circuitous in lead I but positive in lead Two.
- Left axis difference: Net positive QRS complex in lead I but negative in atomic number 82 Two.
- Extreme axis difference (–90°to 180°): Net negative QRS circuitous in leads I and 2.
Axis divergence: right centrality deviation (RAD) and left centrality departure (LAD)
Causes of right axis deviation
Normal in newborns. Right ventricular hypertrophy. Acute cor pulmonale (pulmonary embolism). Chronic cor pulmonale (COPD, pulmonary hypertension, pulmonary valve stenosis). Lateral ventricular infarction. Pre-excitation. Switched arm electrodes (negative P and QRS-T in pb I). Situs inversus. Left posterior fascicular block is diagnosed when the axis is betwixt 90° and 180° with rS complex in I and aVL also as qR circuitous in III and aVF (with QRS duration <0.12 seconds), provided that other causes of correct axis deviation have been excluded.
Causes of left axis deviation
Left bundle branch block. Left ventricular hypertrophy. Inferior infarction. Pre-excitation. Left anterior fascicular cake is diagnosed if the axis is between -45° and xc° with qR complex in aVL and QRS elapsing is 0,12 s, provided that other causes of left axis deviation take been excluded.
Causes of farthermost axis divergence
Rare. About likely due to misplaced limb electrodes. If the rhythm is tachycardia with wide QRS complexes, then ventricular tachycardia is the most likely crusade.
Adjacent affiliate
A systematic approach to ECG interpretation
Introduction to ECG interpretation
Cardiac electrophysiology: action potentials, automaticity, electrical vectors
The ECG leads (12-lead ECG and other pb systems)
Cabrera format of the 12-lead ECG
Video lecture on ECG estimation
Mechanisms of cardiac arrhythmias
Introduction to coronary artery disease (ischemic heart disease)
Atrioventricular cake (AV block)
Right bundle branch block
Left bundle branch cake
View all chapters in Introduction to ECG Estimation.
Source: https://ecgwaves.com/topic/ecg-normal-p-wave-qrs-complex-st-segment-t-wave-j-point/
0 Response to "what term is used to describe the portion of the graph where the waves overlap"
Post a Comment